
Vertebral compression fractures (VCF’s) are the most common osteoporotic fragility fractures. They have an incidence in the United Kingdom of 120,000 per annum (1). VCF’s are considered a red flag pathology of the spine due to the devastating consequences (albeit rare) they can have upon the patient’s health (2). Their true prevalence is likely underestimated, as up to 75% remain asymptomatic but is likely to increase because of an ageing population with a third of women and 20% of men >50 years experiencing an osteoporotic fracture in their lifetime (3, 4).
The aim of this blog is to improve your understanding with:
- Recognising the condition
- Interventions available
- Referral considerations
These are skills which I believe are imperative. Especially considering there has been a steady rise in first contact roles, self-referrals or acute presentation in private practice. So the next time a patient walks in and quotes the infamous Mike Tyson “my back is broken, it’s spinal”, you should hopefully have more confidence with this condition. Before we delve into things, if you want to refine your assessment skills of those with back pain, check out this excellent Masterclass by Dr. Kevin Wernli here.
Recognising VCF’s
- Having a VCF increases the risk of a further one five-fold (3)
- 2-3x more likely to suffer a hip or other fragility fracture (3)
- Associated with the presence of osteoporosis (3)
- Increases risk of neck pain due to altered spinal posture
- Severe cases may impede respiratory function due to marked kyphosis
- Cosmetic dismay for some
- Impaired sagittal balance, subsequently increasing risk of falls (6)

Therefore, although acute presentations may offer minimal issues, the long-term ramifications may cause a headache for clinicians and patients alike. So how do we go about increasing our clinical suspicion of VCF’s? Well, the devil is in the detail; allocating time to review both medical and drug history will provide an insight towards ones bone health before even setting eyes on the individual. Some of the risks include:
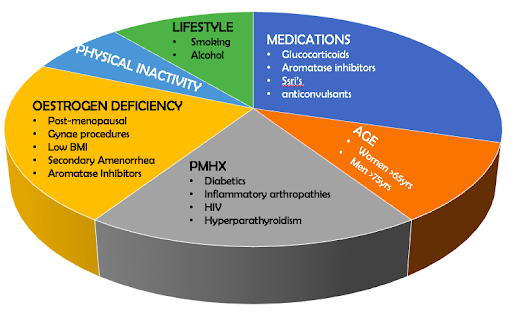
A little bit more around certain risks;
Glucocorticoids
Their use is thought to reduce bone mineral density by 12% within the first year. Approximately 50% of chronic steroid users experience an osteoporotic fracture due to its deleterious effects on osteoblast activity with just 5mg prednisolone daily for 3/12 being enough to elicit these effects (3, 7).
Oestrogen Deficiency
Oestrogen plays a pivotal role in bone health through; a) reducing inflammation, b) reducing osteoclast activity, c) increases production of calcitonin and more (8). Conditions such as menopause, RED-S and medications like aromatase inhibitors will suppress oestrogen production.
Subjective Clues
Patients may describe an inciting event which appears innocuous without trauma and through daily chores; lifting, sneezing or turning in bed (3). Pain can be localised, but may refer towards the ribs, groin, buttocks and hip in over two thirds of patients (11).
Objective Features
Up to 75% will occur at the thoracolumbar junction between T12-L2 due to axial load going through a fairly mobile vs fixed segment of the spine (9). Approximately half will occur anteriorly, these are known as wedge fractures and are usually stable. They occur secondary to stress shielding via the posterior segments; therefore being less robust to withstand compressive load (3). Some of the tell-tale physical features may include:
- Kyphosis and increased postural instability in advanced cases
- Difficulty or inability to lie supine OR sit in a hard chair
- Tender with percussion over corresponding segments (10)
- Paraspinal contracture secondary to pain and attempts to maintain upright posture
Management Options
Education
The majority of VCF’s have a promising natural history, so whether you are a glass half full or empty clinician, the outlook is usually optimistic. Often patients will have marked improvement within six weeks and rarely will complications such as neurological dysfunction occur (6). This is supported through other longitudinal studies that found over half had good pain relief with conservative rehab after three months (12).
Relaying this information is important, as even uttering the word ‘fracture’ has similarities to Voldemort, sending shivers up the spine (no pun intended). However, navigating difficult conversations and informing patients that 40% may develop persistent pain (especially if minimal improvement within 3/12) is also important for three reasons:
- Shared decision-making,
- Medico-legally and
- To inform onward investigations (12).
We must also discuss the other ramifications associated with VCF’s on future morbidity and disability outlined above. Here I find outlining a plan B and C can be effective to help provide reassurance that if things don’t go to plan, there are other options.
Lifestyle Choices
As physiotherapist’s we are well equipped at addressing detrimental behaviour choices because we tend to have the luxury of time and recurrent visits compared to our medical colleagues. Here, collaboratively working towards implementing healthier lifestyle options can have an advantageous effect on bone health and reduce the risk of further osteoporotic fractures. Examples include (3);
- Smoking cessation
- Reduction in alcohol
- Promoting regular physical activity (ideally weight-bearing)
Exercise
Fortunately, gone are the days whereby patients were ill advised on bed rest and discontinuing activity. We now know that regular and progressive weight-bearing exercise (without exacerbating symptoms) improves strength and balance. This is advantageous towards bone health and decreasing the risk of falls, reduced mobility and sarcopenia (3, 13). Initially refraining from activities which evoke pain like repetitive or end range spinal movements are sensible until symptoms are under control but once this settles, patient’s should be given the green light to commence exercises like:
- Balance – single leg stand > tandem stance > tight rope walking
- Weight-Bearing – marching > jogging on spot > pogo jumps > skipping
- Strengthening – wall press > squats > bridges > lateral raise
For further information, I would signpost you towards the Royal Osteoporosis Society which has extensive resources to provide to patients.

Bracing
There is limited evidence regarding its efficacy. However, it might be advantageous for improving pain and self-confidence during activity by limiting spinal movements, thus creating the sensation of increased stability (3). There are several which can be used and this is dependent on fracture location. One risk to be mindful of are pressure ulcers and both clinicians and patients alike should continually monitor for changes in tissue viability (14).
Pharmacology
A large percentage who suffer from VCF’s are elderly and suffer medication-induced side effects. A stepped approach with regards to analgesia is recommended, starting with the most risk averse and progressing if necessary (3). Supplementation in the form of Vitamin D and Calcium can have a positive influence on bone health via intestinal calcium absorption and maintenance of architecture respectively (15, 16). Additionally, antiresorptive agents (oestrogen, bisphosphonates) are recommended for VCF’s; they work by decreasing bone resorption. They do however come with side effects and it is important all cautions/contraindications are considered prior to commencing (16).
Referral Considerations
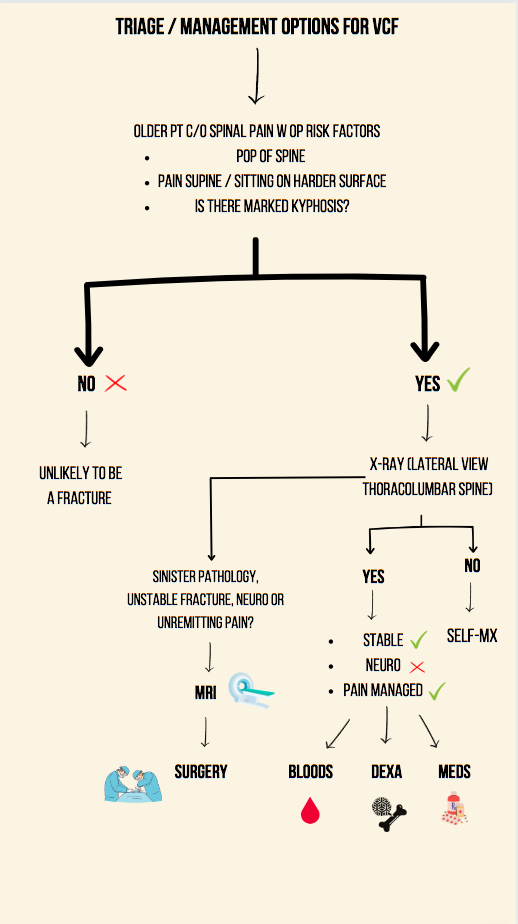
So, after all this waffling, what is the best way to approach VCF’s? Well, there isn’t a cookie cutter approach and each scenario will have its own unique complications but hopefully this provides a flavour as to how I would consider managing it. See diagram below:
A VCF warrants diagnostic work-up as their presence will;
- change bone health classification,
- influences future fracture risk and
- heavily influences treatment selection (3).
Examples include:
Imaging:
Lateral radiographs of the thoracolumbar spine can help identify fractures. The caveat is that ascertaining acute vs chronic via x-ray is challenging. More advanced imaging in the form of MRI has much better sensitivity and can be used for:
- Suspicion of neurological involvement
- Concerns of malignancy
- Fracture instability
- Identifying acute fracture through increased oedema on STIR / T2 imaging
Neurological Involvement
This increases suspicion of a large/unstable fracture which may have retropulsed into the epidural space, also malignancy or infection (3). A thorough subjective and objective screening will help you decide. If concerned, this warrants an MRI accompanied with a neurosurgical opinion.
Laboratory Tests
Unfortunately, a VCF can be the first sign of malignancy and 10% of these metastasise to the spine, often causing fractures (3). There is also a catalogue of endocrine disorders which may result in secondary osteoporosis. The National Osteoporosis Foundation recommends a battery of tests to help identify any underlying medical pathology. This will be down to a doctors discretion but some include:
- Serum protein electrophoresis + Bence Jones Protein (Multiple Myeloma)
- Bone Profile tests
- Renal & liver function
- Thyroid function tests
- Full blood count
- The list goes on….
DEXA Scan
This examines bone mineral density (BMD). Osteoporosis is defined as a BMD of <-2.5 SD of a value for young healthy individuals (16).
Fracture Risk Assessment Tool Model (FRAX)
This can predict future fracture risk over ten years.
Surgery
This is typically reserved for recalcitrant cases, scenarios would include:
- Intense/unremitting pain
- Inadequate symptom relief after 3/12 of conservative efforts
- Presence of neurological compromise
- Stabilise fracture and reduce risk of further vertebral collapse
There are different techniques which can be adopted such as vertebroplasty, kyphoplasty and spinal fusion (the details of which are this blog post), but the former appears most popular. Its efficacy is questionable as studies have illustrated it does not outperform sham for alleviating pain (17). It does, however, appear to be effective for acute, severely painful presentations as vertebroplasty outperformed lidocaine injection for improving pain and disability both acutely and up to 6/12 post-intervention (18).
Wrapping up
To summarise, VCF’s are common and although they rarely produce symptoms, diagnosis matters because of the long-term health consequences associated with them. Most of your suspicion will come from the subjective and patient’s medical history. If confirmed and painful, liaise amongst your medical colleagues to provide analgesia and diagnostic work up whilst mother nature does the rest. If confirmed and accompanied with concomitant risks +/- red flags, utilise relevant secondary care or acute services for advanced imaging, medical management or potentially surgical intervention.
Simple, aye?
If you found this useful, I think you’ll love this Masterclass by Dr. Kevin Wernli on all things related to back pain, movement and posture here.
Want to become more confident treating low back pain?
Dr Kevin Wernli has done a Masterclass lecture series for us!
“Low back pain, movement, and posture… how do they relate?”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!