
Introduction
Anterior knee pain (AKP) has many definitions and is often used as an umbrella term for pathologies that cannot be classified as anything else. The term has been used interchangeably with patellofemoral pain (PFP), chondromalacia patellae, runner’s knee, and patellofemoral syndrome/joint dysfunction.
However, there are a number of conditions that can present as anterior knee pain which I will explore later. The purpose of this blog is to help you differentiate between pathologies that present as AKP, with a specific focus on PFP and Hoffa’s fat pad (HFP) impingement.
Patellofemoral Pain
AKP is most commonly referred to as PFP which is a debilitating condition affecting people of all ages, with a prevalence of 12-13% in women aged 18-35 years (1). PFP is characterised by pain around or behind the patella during weight bearing on a flexed knee. These activities may include walking upstairs, downstairs, hill walking, squatting, kneeling, running, and sitting for long periods.
The aetiology of PFP is unclear and the pathophysiological profile of PFP is multifactorial, with research largely focusing on the anatomical and biomechanical causes. However, some research has shown that symptoms can persist for up to 20 years and there is a strong association between PFP, anxiety and depression (2). Nonetheless, there is also another major contributor to AKP, Hoffa’s fat pad.
Hoffa’s Fat Pad (HFP) Impingement
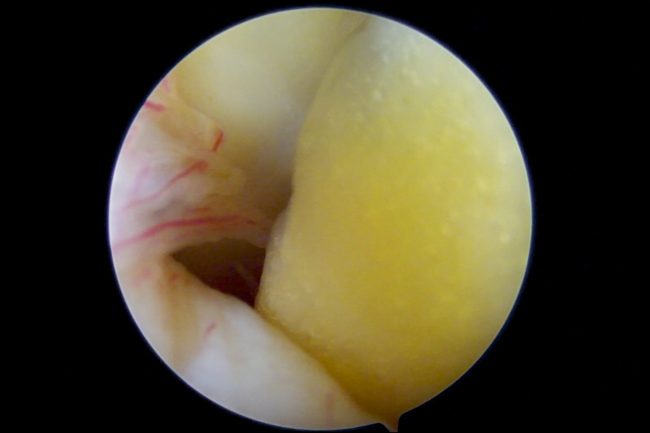
The infrapatellar fat pad (also known as Hoffa’s fat pad, after Albert Hoffa in 1904) is said to be the most sensitive structure in the knee. It is an intracapsular, but extra-synovial structure bounded anteriorly by the patellar tendon and posteriorly by the knee joint (3). Interestingly, its function is not fully understood but it is thought to act as a cushion and to distribute synovial fluid
For some patients, the cause of HFP impingement may be due to chronic compression and irritation, which Claire Patella referred to as ‘’micro trauma leading to a macro problem’’ in her Masterclass on Patellofemoral Pain.
Given its anatomical location and that it is richly innervated with nociceptive nerve fibres, it can be a major source of AKP and co-exist with other pathologies. It also contains adipocytes, macrophages, and immune cells capable of producing inflammatory cytokines suggesting an inflammatory process in HFP. This may be key to understanding the pathophysiology of OA and obesity in AKP.
Hoffa’s fat pad
Osteoarthritis (OA) and Obesity
There is a high prevalence of AKP in patients with OA and obesity (4). Considerable evidence indicates that OA has a multifactorial aetiology with a combination of biomechanical, genetic, inflammatory, and hormonal factors. Clockaerts et al (2010) refers to a study where obese patients reported more symptomatic relief in knee OA with a loss of body fat compared to a loss of bodyweight. This may be explained by the different metabolic pattern in the fat pad which can increase cartilage degradation.
Research has also shown a 23.6% increase in fat pad volume in PFJ OA (5). Therefore, the combination of greater fat pad volume with more inflammation may result in more pain (6). It is no surprise from the above that a mixed picture of AKP can present clinically, making the assessment and diagnosis difficult.
Assessment
When conducting your assessment, it is useful to consider risk factors and potential contributors to AKP (7). Below is a table highlighting some risk factors for PFP and HFP impingement.
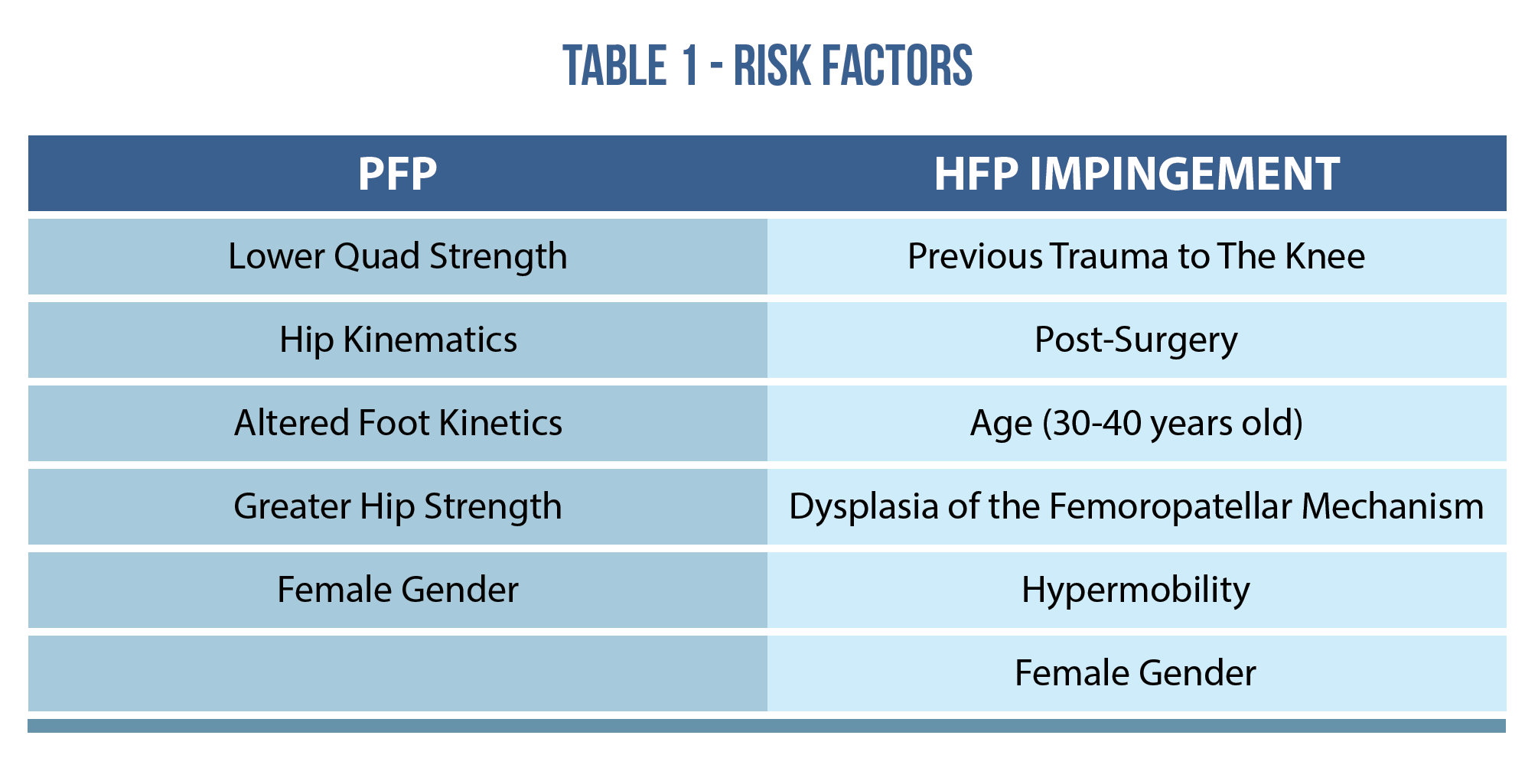
A thorough assessment will help with your differential diagnosis of AKP. Clinicians should actively listen to the patient who may volunteer useful information that can help to differentiate between PFP and HFP impingement. Although the below table makes a binary distinction between the two conditions, remember that the beauty of clinical practice is that they may co-exist.

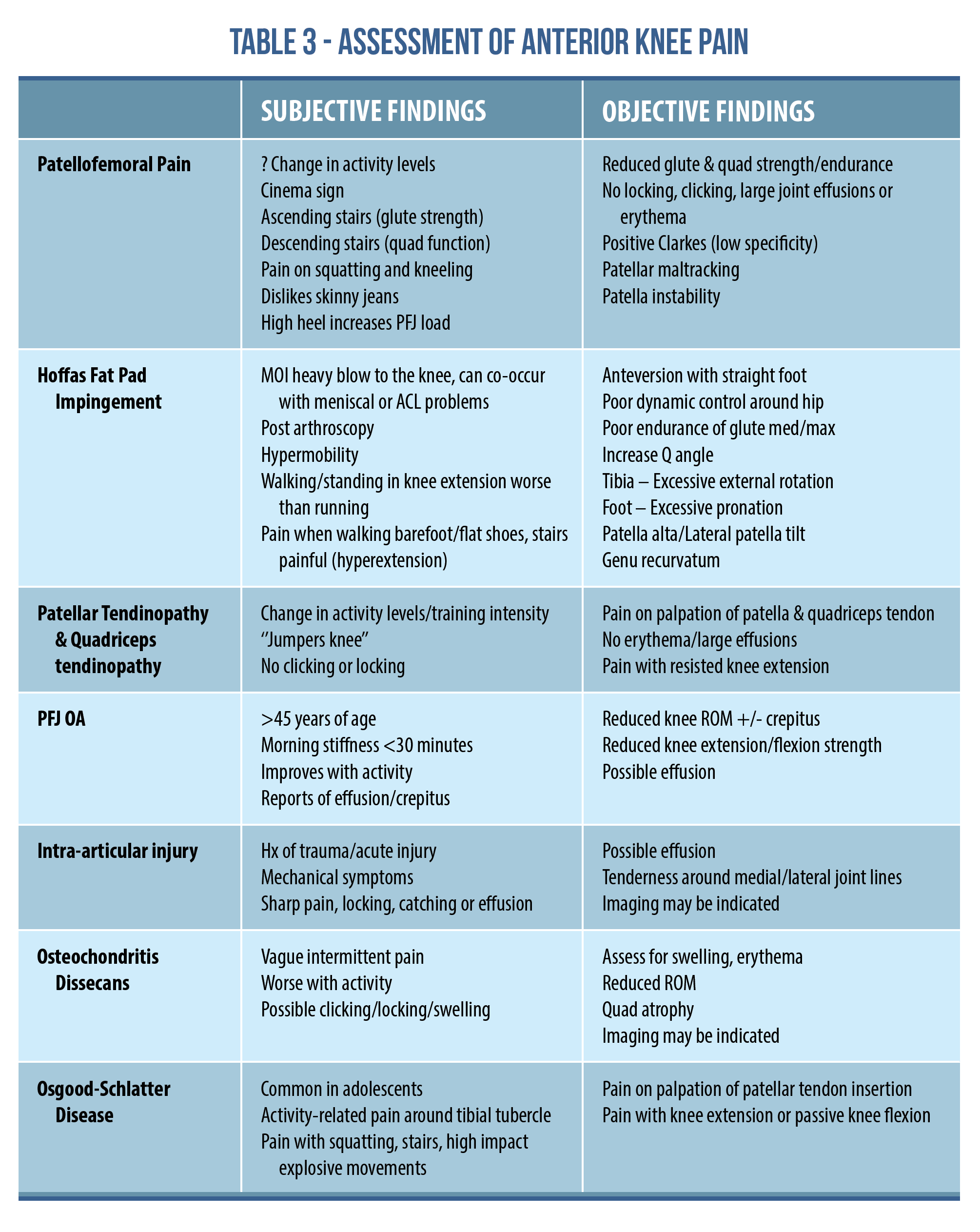
Unfortunately for the clinician, AKP is not just about PFP and HFP impingement, and can have many different aetiologies. The table below outlines several conditions along with the subjective and objective findings that can present as AKP. This is not an exhaustive list, but a brief outline to help clinicians.
Conclusion
This blog skimmed the surface of the differential diagnosis of AKP, with a focus on PFP and HFP impingement. You should now have a better understanding of the signs and symptoms and risk factors of PFP and HFP impingement, and be able to differentiate between the two conditions. Remember that AKP can have many different aetiologies and a thorough assessment will help guide your treatment.
To delve into more detail on the assessment and treatment of AKP, check out Claire Patella’s Masterclass.
Want to learn more about anterior knee pain?
Claire Patella has done a Masterclass lecture series for us on:
“Patellofemoral pain”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!