
If you follow any of the business experts in physical therapy such as Darryl Yardley, Rick Lau or Paul Gough, you’ve likely heard of the importance of booking clients for treatment plans. For us ethically minded clinicians who genuinely care about what we do, the term treatment plan has a very negative connotation to it and conjures up images of people getting thrice weekly appointments from here to eternity. In reality, that’s not a problem with using treatment plans but rather abusing treatment plans.
As someone who uses treatment plans, I want to discuss:
- Why they are beneficial for the patient and are not necessarily just a money grab
- How to plan and set them up as well as how to convey recommendations to the client
On that note, I highly recommend this Masterclass by Dr. Tim Mitchell on a framework for optimizing the patient interview and clinical outcomes . A large part of determining a care plan comes from the patient interview.
Part 1: How do treatment plans benefit the client?
Treatment plans benefit the client by giving the client a clear idea of what to expect and creating confidence in the treatment provided. For example, I could present a weight training client with the the following options:
Option 1:
“I want to see you twice this week and twice next week. We’ll do some exercise and hands-on therapy, see how things go and take it from there.”
Or
Option 2:
“We’re going to spend the first 3 weeks modifying your training to keep you active while settling down your pain, doing hands-on therapy to improve the flexibility and pain in your shoulders, and doing rotator cuff and scapula strengthening to help with pain reduction, strengthening the affected areas, and correcting some imbalances. Twice weekly sessions are ideal.
Then we’re going to spend the next 4-6 weeks gradually building you back towards pressing movements, doing higher level shoulder/rotator cuff strengthening, helping you program and progress your weights so you get back safely, and still doing hands-on therapy but less often. In this case we’ll do a session a week for the first two weeks & then drop down to biweekly then monthly.’’
Which option provides more clarity and inspires more patient confidence?

Now I get that there is a fine line between explaining and not overwhelming the client, but I’d rather provide too much detail than not enough.
Side note: I always recommend having some kind of email or print out that can be given to the client to outline both the treatment plan, home exercises, and any education or tips given. A lot of what we teach is forgotten and/or misinterpreted (1) so having it on paper helps a lot.
1) Having regular intervals to re-measure goals in a timely fashion
One thing I always tell clients on Day 1 is how often goals get reassessed. I talk about this more in my article on outcome measures (2).
I always like to take time with each new client to set reminders for when to re-assess certain areas (i.e. pain, strength, rom, ability to do a certain task). This is much trickier to do if clients are not booked ahead, if sessions are missed or if a large gap occurs between sessions. It can make it more difficult to assess progress in a timely fashion and update the program.
2) Enables clients to get preferred times
Anyone who works in outpatient orthopedics will tell you that the evening times are always the busiest as clients come after work. Booking a care plan further ahead is advantageous as it enables clients to get their desired times.
3) Keeping the client scheduled and on track in case missed appointments occur
This is a big thing during covid times, as it’s not uncommon to see clients miss a week or two of appointments due to sickness or isolating. If you only book a client for a week or two and the client misses a couple weeks due to being sick then it can be a nightmare, and sometimes impossible, to get them back on track. The client falls off and doesn’t reach his/her goals.
Having a plan booked out can help reduce the likelihood of that happening.

Part 2: Setting up a treatment plan
Before setting up a treatment plan there are a couple disclaimers I have:
- Everything is subject to change. I often say “the best made plan doesn’t survive contact with the patient.” It isn’t set in stone.
- Here, I am discussing what I recommend to clients for a plan. The actual plan may need to be adjusted based on finances, scheduling and/or other factors.
Side note: one mistake I used to make, and see providers make on a regular basis, is basing treatment recommendations (note I said recommendations) around benefits rather than what the clinician feels is right. If 6 sessions is right, that’s fine. If 36 sessions is right, that’s fine. I always tell patients that I recommend what I think is ideal and then we adjust from there & would rather do that than presume and undershoot.
1) Frequency of sessions
The frequency of sessions that I recommend comes down to five factors:
- Is the client progressing?
- A client who’s almost fully recovered and just needs high level strengthening and workload management to help address achilles pain in the fourth quarter of a basketball game can be followed up every few weeks or less.
- In contrast, I have a hard time doing sessions <1 time per week with a client who is more up & down.
- How closely does the client need to be monitored?
- The above basketball player likely doesn’t need a lot of close monitoring and can have a much lower treatment frequency, if he is only having pain during the 4th quarter.
- In contrast if you have a client who:
- Has a symptomatic disc herniation and feels good in the clinic and good with extension but bends his/her back a lot without realizing it which affects progress.
- Or someone who has more of a central sensitization pattern, fear avoidant, and shudders away from exercise due to pain, than a higher treatment frequency makes sense.
- How much need is there for manual therapy to regain ROM?
- I use manual therapy, but predominantly to help regain ROM rather than pain relief. Therefore:
- A post op limb, particularly a stiff one, may need multiple sessions per week to regain ROM.
- On the flipside a client who has full ROM may not need to be seen as frequently.
- I use manual therapy, but predominantly to help regain ROM rather than pain relief. Therefore:
- How fast can you progress exercises?
- A young, healthy and active client may be able to progress exercises even multiple times within the same week.
- In contrast, an older, less healthy, deconditioned client may need a few weeks before they are ready to progress exercise difficulty.
- Side note: in these situations where progress may be slow and patients may be stuck doing the same exercise routine for a long period of time, it is critical to set expectations on Day 1. This helps to anticipate the individual’s frustration with slow progress.
- How time sensitive is the goal?
- If the client is preparing for a big trip or a sporting event in a few weeks, it certainly makes sense to book them for multiple sessions per week.

2) Length of treatment sessions
Depending on where you work, it may be the case that each client has the same amount of allotted time for an appointment but if you work in a setting where you have flexibility in how you schedule appointment times for each patient, the length of treatment sessions is worth considering.
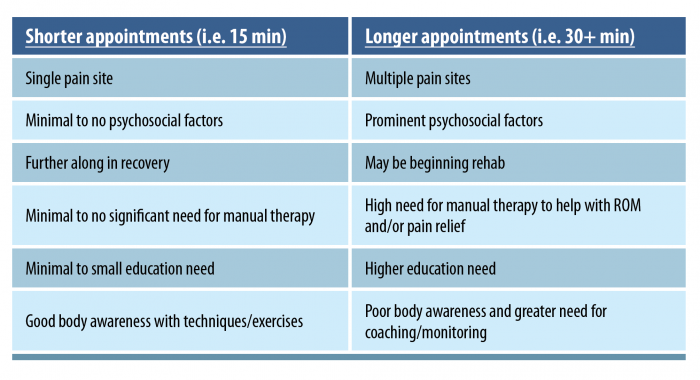
Not everyone needs a thirty minute appointment. A client who has a hamstring strain, has a high level of strength and balance, is pain free in everything except high level martial arts, may not need a thirty minute appointment. A fifteen minute appointment for a quick check-in and a bit of exercise tweaking, education on workload management and as-needed manual therapy may be all that’s needed. However, a client who has near constant pain in four different areas along with a high level of distress and psychosocial factors may benefit from a 45-60 minute appointment.
In general I use the following guidelines when deciding whether or not to book clients for longer or shorter treatment appointments:
3) Components
This is where things like the following are important:
- Exercise to help with strength, mobility, return to activities, injury reduction and pain
- Manual therapy to help with pain relief and improving mobility in the affected and/or neighboring areas
- Education on pain and hurt vs harm, pain management and how to return to activities
The key is to tie in how all these are relevant to the individual’s goals. If a patient or coworker asks you why that treatment is included and you don’t have an immediate reason why, then that can be a big problem.
4) Reassessment of goals
It’s important also to communicate when goals are reassessed. I usually use the following as a guideline:
- ROM: every session
- Pain: every session if acute or less complex; every few weeks if chronic or more complex
- Strength: every 2-12 weeks depending on expected rate of improvement.
- Ability to do goal tasks. This takes a few different forms:
- If it’s a task the client is already doing consistently but not fully, I’ll usually ask each session how much of it the client is doing and get them to track it.
- If it’s more a self-perceived ability to do it (i.e. a Patient Specific Functional Scale questionnaire) I’ll usually do that every few weeks.

I set reminders in the appointment notes on when to reassess things. This ensures progress is being reassessed and the program is updated in a timely fashion.
5) Referrals
This can include, but is not limited to, such things as:
- Mental health providers (i.e. psychology, psychotherapy, psychiatry)
- Nutrition professionals (i.e. dietitian) for help with weight loss, or other nutrition questions.
- Fitness professionals if a more general weight loss program is needed, if they have fitness or performance goals that are outside of the scope of rehab
I put this all on a handout for the client.
Part 3: Barriers to treatment plans
1) Time to map them out
Mapping out a proper treatment plan can take some time. This can be tricky if you have a complex assessment with a complex client who may have multiple body parts involved, a lot of needs/concerns to address and/or a language barrier.
My argument is that taking the time to discuss and map out the plan now can save a lot of hassle later.
If assessment time is short – focus on what you need to focus on to get a proper diagnosis & rule out red flags while listening to the client properly. I often ask clients “are you OK if we assess X and Y today and leave Z for another time? I want to make sure we’re managing these areas effectively” and clients are usually on board with that.
2) Patients/clinicians not wanting to book that far ahead
It’s pretty common for clinicians to book clients out a couple visits or a couple weeks ahead. This is OK in certain circumstances. For example, if you have a patient who is retired or has flexible work hours and can easily come through the day, but in most cases this isn’t always doable.
Sometimes patients, particularly ones who are on the road or work inconsistent hours, may not always know their schedule that far ahead.
Some clients may want to only book one as they:
- Just want to see how it goes and book back if needed
- Expect to be fixed right away
- May be limited by scheduling, budget, travel, or other factors
And sometimes, let’s call a spade a spade, sometimes the clinician is not a good fit for the client or vice versa.
These can be tricky barriers that are not easy to sort out. I’ve found explaining the plan in detail, the importance of booking ahead and setting realistic goals makes a big difference.
3) Clinician confidence
Sometimes the thought of booking a plan can make clinicians feel like they are (or being seen as) just “in it for the money” or “looking to keep the patient for a ton of appointments.” This isn’t an easy hurdle to overcome.
The best way I’ve found to deal with this is simply to map out the treatment plan and explain the rationale for everything. This shows both the client what to expect and will create confidence for both the clinician and client in the plan.

Sometimes, especially for new grads or therapists not very knowledgeable in a specific area, base knowledge can be a problem. This is where you either have to:
- Look things up (courses, research etc)
- Ask more experienced clinicians for help
- Refer the client to those clinicians
It’s pretty tough to confidently and competently book treatment plans if you aren’t knowledgeable in what you are seeing. In a perfect world we’re all experts in everything, but that isn’t how it works with many areas of physiotherapy. It’s impossible to be super-knowledgeable in orthopedics, sports rehab, pelvic health, chronic pain, stroke rehab, spinal cord injury and pediatrics.
4) Uncertainty of outcome and progression
This is a very valid one. We’ve all had those clients where we’ve thought “OMG what am I gonna do with this person” and then had them come back much improved the next day. We’ve also had those clients who seem super-straightforward and don’t progress very well.
Booking plans ahead can be tricky in clients with:
- Chronic pain
- Multiple injuries/comorbidities
- Very high return to play or return to work goals
- Experiences with past providers
There are so many factors that influence pain that we cannot predict how a client will respond with 100% certainty and it isn’t practical to book 4-6+ months ahead.
In this situation my only recommendation is to book out for a reasonable length of time (1-3 months) and educate them that the recovery timeframes can be long & variable.
Wrapping up
I hope this blog helps provide some guidance with setting up treatment plans. Do you use treatment planning in your own practice? If so, leave a comment below on how you set them up. For more depth on optimizing patient outcomes, check out Dr. Tim Mitchell’s Masterclass here. As always, thanks for reading.
References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!