
Hopefully by now you know that reconstruction is not the only way to deal with ACL injuries. There is robust evidence to show that those who are conservatively treated are at no higher risk of OA and other sequelae (Ref,Ref). And hopefully, it is not news to you that you can even return to pivoting sports without having an ACL injury surgically managed (Ref, Ref). I’m not, however, here to argue the merits of conservative versus surgical management. Through this blog, I will contend that the most important first step is to improve the pathway immediately after an ACL injury. From there we can begin to understand when the surgical route needs to be undertaken (non-copers), or conversely in what population group surgery can be avoided (copers).
Houston.. we have a problem.
ACL injuries are responsible for a significant societal and economic burden and this might surprise you, but reconstruction is shown to result in cost savings compared to conservative rehabilitation (Ref). We are also, however, seeing revision reconstructions increasing at a rate of knots per year (Ref) and it seems if it were as simple as ‘reconstruction works’ then this probably wouldn’t be an observable trend. Us physios, unfortunately, continue to do a pretty poor job at ACL rehabilitation (Ref), but that can’t explain the explain the entire problem. Possibly it should be ‘reconstruction works, in the right people, after the right pre-operative pathway’. In countries with national registries and nationally applied pathways following ACL injury, reconstruction rates are much lower; saving health dollars but also helping patients avoid unnecessary (traumatic) surgery (Ref). I’ve had 2 ACL reconstructions, so believe me, I know they can be traumatic.
In Australia in particular we have one of the highest rates of injury in the world, the highest reconstruction rates, a rapidly rising youth reconstruction rate (those under 14 years old) and no national registry – it is literally the Wild West of ACL injury (Ref,Ref). I’m worried about the future of our youth athletes and you should be too.
Like all things, there is no one size fits all and there is plenty of grey.
Copers and non-copers currently defined.
It is worth stating, that currently, there is no known way to identify copers following an ACL injury (Ref). But for those with an ACL deficient knee, potential copers are characterized as having good knee stability and the ability to compensate well after injury, whereas noncopers have poor knee stability and less potential for compensation.
So what exactly makes up a coper?
A short synopsis of the (very low quality) research goes as follows:
- In really simple tasks like walking, there is potentially increased hamstring activation in chronic (ACL injury >6 months ago) copers compared to non-copers (Ref). This might seem to make intuitive sense, in that there may be a ‘compensatory’ mechanism going on here.
- There is some data that non-copers intuitively ‘protect’ the knee by reducing their extensor moment in gait (Ref).
- Surprise, surprise – quadriceps inhibition and loss of size was found as a common factor in all non-copers in some low quality studies (Ref, Ref).
- Kinesiophobia levels would seem to be higher immediately after ACL injury in noncopers (Ref).
Caution! It would be wise to not make any conclusions about your patients based on the above data. In a multifactorial and complex condition like ACL injury there is little use in predicting the outcome from some simple initial data. A much better way forward is to ‘probe, sense, respond’ as you would with any other complex condition.
The current world best-practice model recommends an initial physical rehabilitation program for 3 months (called prehabilitation) (Ref). It is only then that you can classify someone as a coper or a non-coper.
Currently, the best definition of a ‘coper’ is provided by the following criteria, proposed by Wendy Hurd and team in 2009 and since applied successfully by Wellsandt et al (2018) in a large cohort (n=105):
- A timed hop score of ≥ 80% of the other side
- A Knee Outcome Survey-Activity of Daily Living Scale (KOS-ADLS) score of ≥ 80%
- A global rating score (GRS) of ≥ 60%
- ≤ 1 giving way episode since the injury (Ref, Ref)
This period of initial rehabilitation is then followed by a shared decision-making process to undertake a non-operative or operative management pathway. Considerations informing this decision are very individual and include but are not limited to, desired level of sporting participation, functional knee stability, occupational requirements, financial and time restraints and patient and practitioner knowledge and beliefs.
What does immediate ‘prehabilitation’ look like?
A really simple, clear 5-week pre-operative rehabilitation program initially proposed by Eitzen et al (2010)is called the Norwegian Research Centre for Active Rehabilitation (NAR) programme (it is freely available to view). In a prospective cohort study by Grindem et al (2015)(n=84), those that underwent this pre-operative rehabilitation fared better in all Knee Osteoarthritis Outcome Score (KOOS) subscales (Pain, ADLs, Sports and QoL) in comparison to a control cohort.
The rough outline to an immediate prehabilitation programme looks like so:
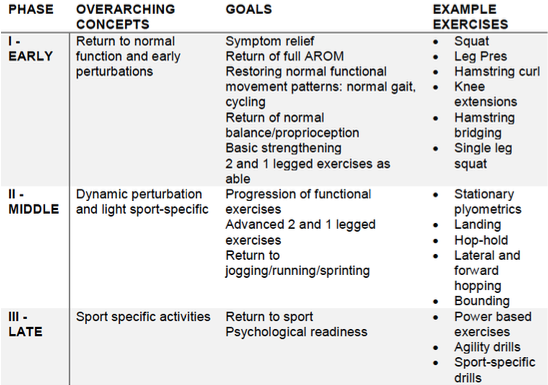
Ref: @CG High Performance
The addition of perturbation trainingis recommended FROM DAY 1 in all ACL injured patients, so if you aren’t doing that it might be time to start (Ref, Ref). An example of a simple perturbation program can be found here.
Putting it all together.
So, if you aren’t going to ‘identify’ a coper early post-ACL injury and world best-practice guidelines recommend for EVERYONE to undergo an initial evidence-based rehabilitation program, then I ask physios reading; why aren’t we all doing this?
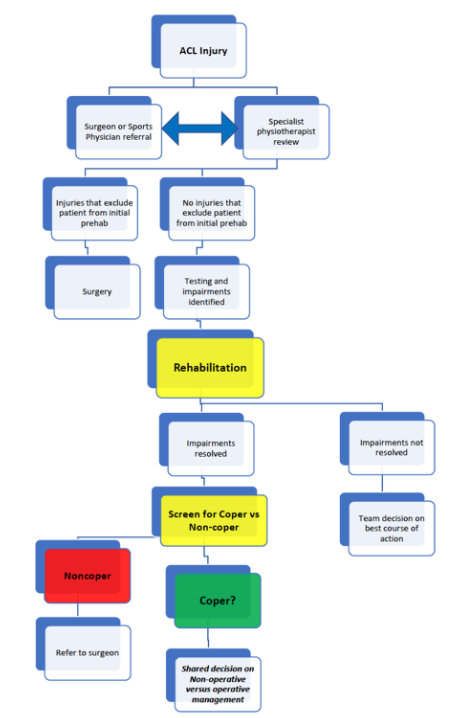
I’ve adapted this decision matrix from Hurd et al 2009:
Does coping predict future success after ACL reconstruction?
There is now some evidence to show that improving the patient’s potential coping status improves post-operative outcomes (Ref). But what is more important, is that up to 2 years after ACL reconstruction, those treated with an extended period of pre-operative rehabilitation – the Delaware Oslo Cohort (n=150) – fared much better in IKDC, KOOS and had a significantly higher rate of return to sport than those who didn’t (Ref).
And it seems that once again, failure to regain adequate (>90%) quadriceps symmetry pre-operatively can have the potential to predict future RTS success (whether they will actually pass RTS criteria) (Ref). This makes intuitive sense, as it has been shown that you lose much quadriceps strength after ACLR anyway, so if starting from a lower base, you finish lower (Ref). Noncopers also seem to take longer to pass return to sport criteria following ACLR (Ref).
I think the salient point, however, becomes like anything we try to predict in the sporting or musculoskeletal realm; it’s bloody difficult. And the best chance we can do is adhere to certain stringent criteria along a structured pathway and attempt to reduce risk the entire way along this pathway. Once you have put your patient through a structured rehabilitation prior to any surgical decision, you will arrive at the important point; does this person actually require surgery or not?
A word on psychological ‘readiness’
The importance of psychological readiness to return to sport is becoming more apparent (Ref) and given that the studies involving a pre-operative rehabilitation program tend to demonstrate an improvement in subjective knee scores (KOOS, IKDC) then it could be entirely possible that this process is an important one for reducing fear levels and kinesiophobia AFTER reconstruction. There is no evidence available to back up this hypothesis, but I would think progressing through a rigorous, criteria-driven pre-operative rehabilitation program in which athletes are really tested and must meet high-level benchmarks would be providing the psychological ‘graded exposure’ that they may need in returning to sport – whether or not they receive a reconstruction is then simply ‘par for the course’.
We need to do better; a conclusion.
I hope it is obvious we have a big problem on our hands. A problem for which the solution needs to be complex and involve multiple levels of clinicians, stakeholders and most importantly patients. There can’t be a one size fits all solution and just reconstructing everyone’s ACL doesn’t seem to be working now does it? It certainly hasn’t helped everypatient, it hasn’t helped our health system dollars and it’s made us physios look kind of bad (depending on your perspective, this might be a good thing..?). Into the future, this problem will be hitting our youth athletes hardest and causing a significant burden if something doesn’t change. In order to effect change, I will leave you with a few key takeaways on what we need:
- A concerted effort for everyone to become more aware of current evidence regarding the nuances of ACL injury and rehabilitation.
- Clearer national level guidelines and pathways for practitioners in the immediate post injury stages to guide decision making.
- Shared decision making instead of unilateral decisions based on General Practitioner referrals.
- More structured rehab approach both pre-operatively and post-operatively.
- Criteria driven rehabilitation and prehabilitation post injury.
- Less fear amongst physiotherapists and more willingness to push patients to achieve excellent outcomes.
- As always, more research into the above areas to define the problem and to provide information – based on clinical input – on what works and importantly what doesn’t.
Once again, thanks for reading.
Want to get better at treating ACL patients?
Dr Hege Grindem has done a Masterclass lecture series for us on:
“Assessing, managing & rehabilitating ACL injuries”
You can try Masterclass for FREE now with our 7-day trial!

Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!