Morton’s Neuroma – It’s like Walking on a Stone!

‘’A lot of the time it feels like I’m walking on a stone. I feel a burning sensation in some of my toes and it’s definitely worse when I’m walking around barefoot’’.
For those clinicians who work with foot and ankle pathologies, you would have definitely heard the above narrative from a patient. Let’s delve deeper and look at this pathology that is sometimes dismissed with the clinical reasoning of ‘your footwear must be wrong!’
Before we learn about what Morton’s Neuroma actually is, If you want to learn more about the differentials of foot pain, check out this masterclass by Dr. Henrik Riel here.
Who the hell is Morton?
Morton’s neuroma was first described in the literature in 1876 by an American surgeon, Thomas George Morton.
‘Morton’s neuroma’ may represent an over-simplification of the clinical condition and may be misleading for clinicians and patients. It is important for clinicians who deal with this condition to realize that the problem is not a benign tumour of the nerve (as the terminology would imply), but a neuropathic pain in the forefoot that is associated with the interdigital nerve (most commonly the one between the third and fourth metatarsal heads), and to educate their patients accordingly.
It is also referred to in different literature and countries as Morton metatarsalgia, interdigital neuritis, Morton entrapment, interdigital neuralgia, interdigital nerve compression syndrome, and intermetatarsal neuroma. Confused? Don’t worry…keep reading.
The classical description of a Morton’s neuroma is paraesthesia within the affected digital nerve, accompanied by forefoot pain and is more commonly seen in females. 17% of patients describe some trauma to the foot resulting in symptoms (1). Morton’s neuroma is common in middle-aged women. The exact incidence is unknown. Rarely, are both feet affected.
The most common characteristic of the pain is burning in nature. Altered sensations and feeling a “pebble in the shoe” is reported by more than 50% of patients. The pain is often exacerbated by prolonged walking, running or other high impact sports, use of tight or high heeled shoes and is reported by runners due to the increased weight bearing through the forefoot (2).
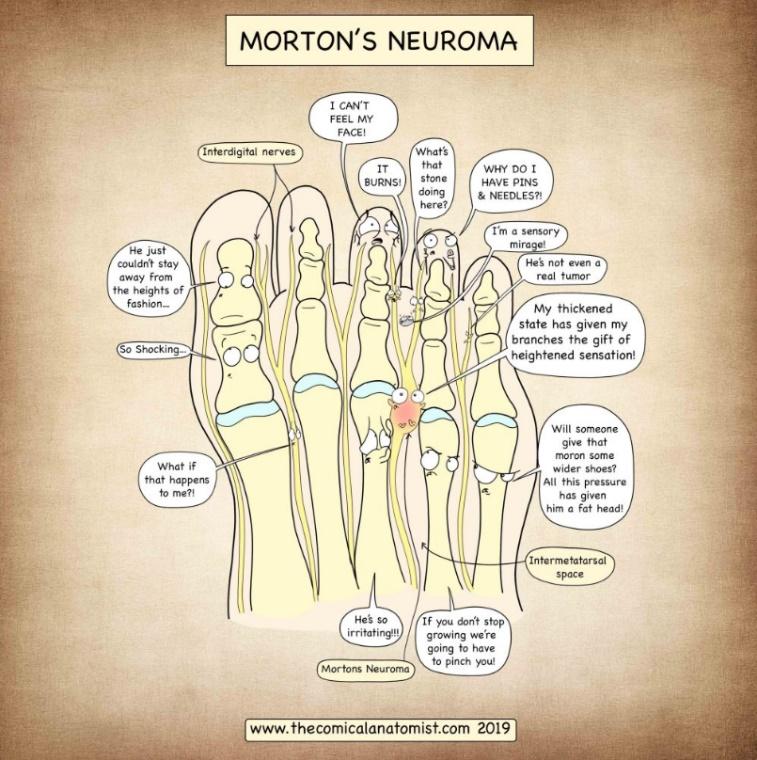
Figure 1 (10)
Resting the foot or removing footwear improves pain in most cases especially early in the onset of this condition. In chronic cases the pain could be constant. Night pain is reported by about 25% of patients. The most common locations for interdigital neuromas are between the 3rd and 4th metatarsal heads (3)
Affecting 88 in every 100,000 women and 50 in every 100,000 men presenting for primary care in the United Kingdom, it is the most common compressive neuropathy after carpal tunnel syndrome (4).
But why does it happen? Can’t just be footwear surely!
Morton’s neuroma is common in the third interspace because it is narrower compared to other spaces. As the common digital nerve to the third space receives branches from both medial and lateral plantar nerves, it has increased thickness and is prone to compression and trauma. Trauma from a crush injury, penetrating injury, thickened transverse metatarsal ligament, enlarged bursa in the interspace, and repetitive trauma from running or dancing have all been linked to the development of Morton’s neuroma (5).
It is the result of altered foot biomechanics and forefoot overload, and the treating clinician must consider the bigger picture which should include load management, existing co-morbidities and biopsychosocial issues as well as wider footwear, metatarsal padding, ESWT, manual therapy and injections. History, clinical presentation and examination usually reveal the diagnosis, whereas imaging studies (standing radiographs, ultrasound, MRI scans) aid in the differential diagnosis process.

What could be the differentials?
Clinically, there are no visual cues to the presence of a neuroma. Any deformity of the foot specially hallux valgus can lead to overcrowding of the toes and increased pressure on the lesser toes, and is therefore an important predisposing factor. Inflammatory gout can also be an influencing factor in some cases.
Other differential diagnoses include, plantar plate tear, Freiberg’s disease, stress fracture of metatarsals, RA, OA, ganglion cyst and central metatarsalgia.
Clinical Tricks
To effectively confirm a Morton’s Neuroma a clinician should perform the following tests:
- Web-space tenderness test
- Squeeze test
- Plantar percussion test
According to research by Owens et al (2011), the webspace and squeeze tests were highly sensitive and specific in 92% of patients (6).
The solution?
The management of Morton’s neuroma can be split into non-surgical or surgical management. The treatment algorithm generally involves non-surgical measures including physiotherapy and injection therapy and if these methods fail to improve symptoms, surgical excision is the next option. Patient education is very important and the use of wide toe box shoes can be the simplest method of managing symptoms. However, patient compliance is an issue and can result in failure to resolve symptoms. Often, a shared decision making process is needed with other healthcare professionals, including podiatrists, sports medicine physicians and orthopedic surgeons.

Managing patient expectations is key. The patient should be educated about the variable success rates of physiotherapy, activity modification, load management, using appropriate footwear and the role of other modalities such as injections and cryotherapy. When surgery is being considered, a significant minority of patients report worsening pain after surgery (7), however, good to excellent results with neuroma excision have been reported in 70–80% of patients (8).
A patient’s description of activity-related, sharp, burning pain with or without paraesthesia, and the feeling of ‘walking on a stone’, together with positive web-space tenderness and forefoot squeeze tests, is indicative of the diagnosis of Morton’s interdigital neuroma. Corticosteroid injections and manipulation/mobilization are the two interventions with the strongest evidence for pain reduction, however, high-quality evidence for a gold standard intervention is not available in the current research (9).
Wrapping up
- Morton’s neuroma is a compressive neuropathy of the forefoot interdigital nerve.
- Diagnosis is usually based on history and clinical examination.
- Imaging can help with masquerading pathologies
- Incorrect footwear is not the main reason a Morton’s neuroma occurs
If you want to learn more about the differentials of foot pain, check out this masterclass by Dr. Henrik Riel here.
Want to become an expert on plantar fasciitis?
Dr Henrik Riel has done a Masterclass lecture series for us!
“Diagnosing and managing plantar heel pain”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!