Exercises for Medial Tibial Stress Syndrome (AKA ‘Shin Splints’)

It’s easy to talk generally with rehab, ‘strengthen x,y and z’, improve movement control etc but we don’t often expand on what exactly this means. Today’s blog is a brief look at an exercise programme I used for a patient with Medial Tibial Stress Syndrome and what my thinking was behind it.
The patient, in this case, is a young male middle-distance runner called Ben. He is, at this stage, pain free with all daily activities and running up to 40 minutes with no symptoms. He’s progressed nicely from the initial session where even jogging on the spot was painful, however, longer runs over 45 minutes cause some discomfort in the medial tibia. This has been a recurrent issue and Ben’s aim is to return to full training without these symptoms. He is gradually re-introducing high intensity sessions with guidance from his running coach and managing well. Assessment reveals mild weakness in Soleus, Glute Med and the posterior chain. Control of single leg balance and single leg dip is good and equal left and right. Ben works with an S&C Coach and is in the gym 3 days per week and is keen to have a number of exercises to work on.
Broadly speaking our aims are as follows:
- Improve local load capacity in the calf complex
- Improve kinetic chain load capacity considering the key muscles that aid in managing load
- Include weight-bearing exercises to improve bone load capacity
- Progress by adding load and/ or impact as this is more likely to stimulate bone adaptation
So Ben’s programme looks like this:
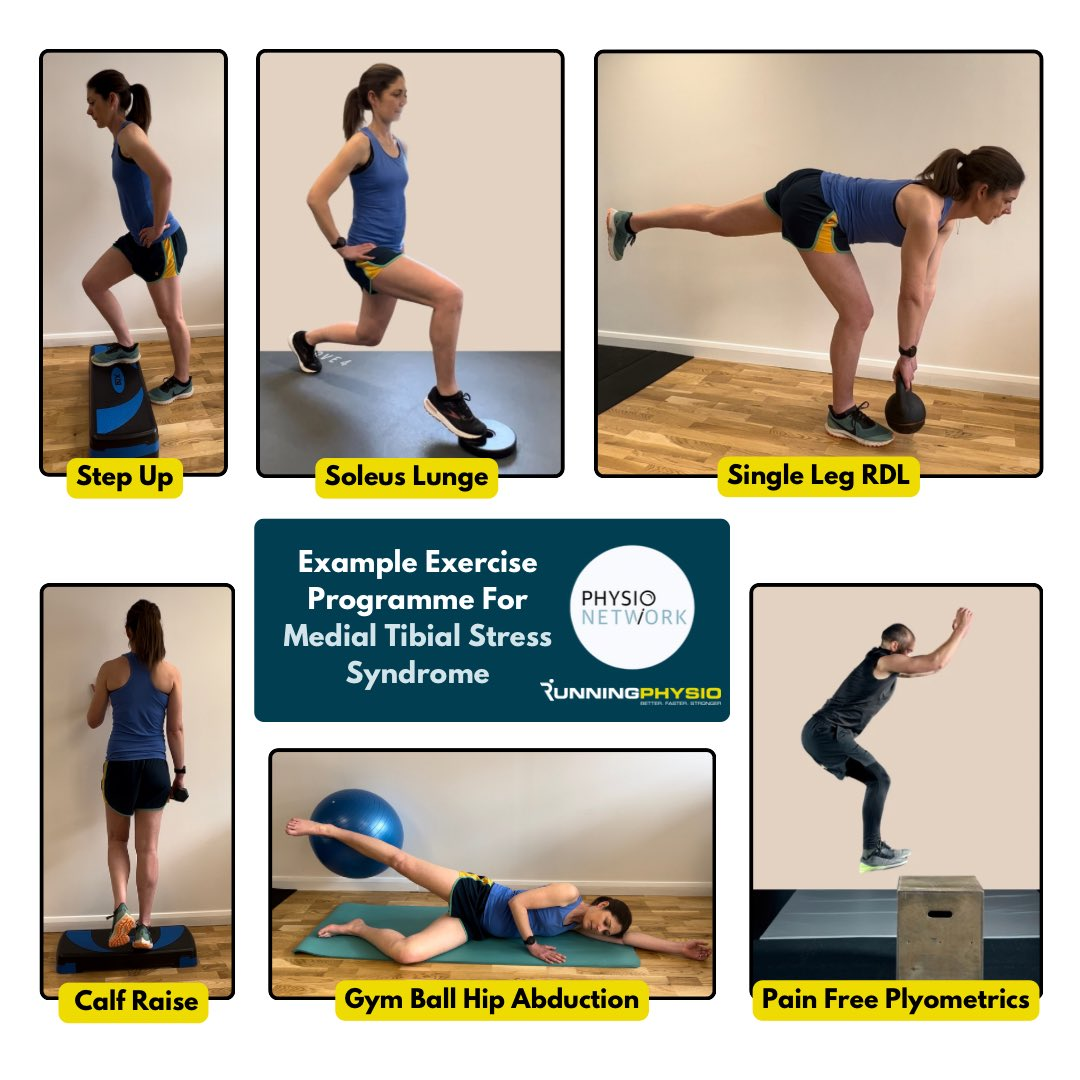
Let’s walk through each exercise.
1. Step ups
Simple but very effective! Step-ups achieve high levels of Glute Max activity (Reiman et al. 2012) as well as working Glute Med and providing a proprioceptive challenge. Gluteal muscles are vital in absorbing load during the stance phase of running. This exercise is first due to control aspect; doing this once fatigued from the other exercises may compromise movement quality. It is easy to progress or adapt to suit the patients changing needs by increasing step height or adding load.
2. Soleus lunge
A nice isometric option that will challenge both the Soleus and Quads – 2 vital muscles in absorbing load during running. Hamner et al. (2010) found the quadriceps to be the greatest contributor to support. In MTSS Soleus is thought to be particularly important as it helps to reduce the bending force that the tibia experiences during impact which is thought to be key to the development of bone stress injury (Warden et al. 2014).
3. Single leg Romanian Deadlift (RDL)
Recent research (Collings et al. 2023) has found that a single leg RDL challenges the whole glutes complex – Glute Max, Med and Min. It also works the hamstrings and challenges balance so has lots of potential benefits.
4. Single leg calf raise
Calf raises (either bent knee or straight) are simple and effective for strengthening the calf which is the major shock absorber at the foot and ankle. Considering the high demands on the calf complex when running it’s often necessary to progress beyond body weight and include additional load. Ben is a forefoot striker and research indicates higher loads for the calf complex in this group (Almonroeder et al. 2013). We want to ensure he has adequate strength to manage this load.
5. Gym ball abduction
Ben’s assessment revealed Glute Med weakness and this is hoping to address this. The gym ball helps recruit Glute Max and reduce compensation from hip flexion. We have weight-bearing exercises like the RDL and step up that will work the Glutes alongside other muscles. The aim of this is a more isolated Glutes workout and trying to work to fatigue to address Ben’s strength deficits. I include this at the very end as once you’ve worked the glutes to fatigue it makes control of other exercises very challenging!
6. Pain free plyometrics
Medial Tibial Stress Syndrome is considered a bone stress injury. Current thinking in such injuries is that they should be pain free both during and after exercise (Warden et al. 2021). This is especially important with impact as this is often most provocative. Plyometrics may be done in a stand alone session or prior to strength work if well tolerated by the patient. It’s best for patients to warm up first to prepare the body for impact.
Despite their potential to aggravate, plyometric exercises can be very effective in stimulating bone adaptation and improving load tolerance. Typically the prescription in BSI is for short duration, explosive work separated by rest. Initially this might be 40 foot contacts or less in the session. It can then be progressed in intensity (providing it’s safe and appropriate for the patient and remains pain free) by increasing speed, jump length/ height, external load or changing direction.
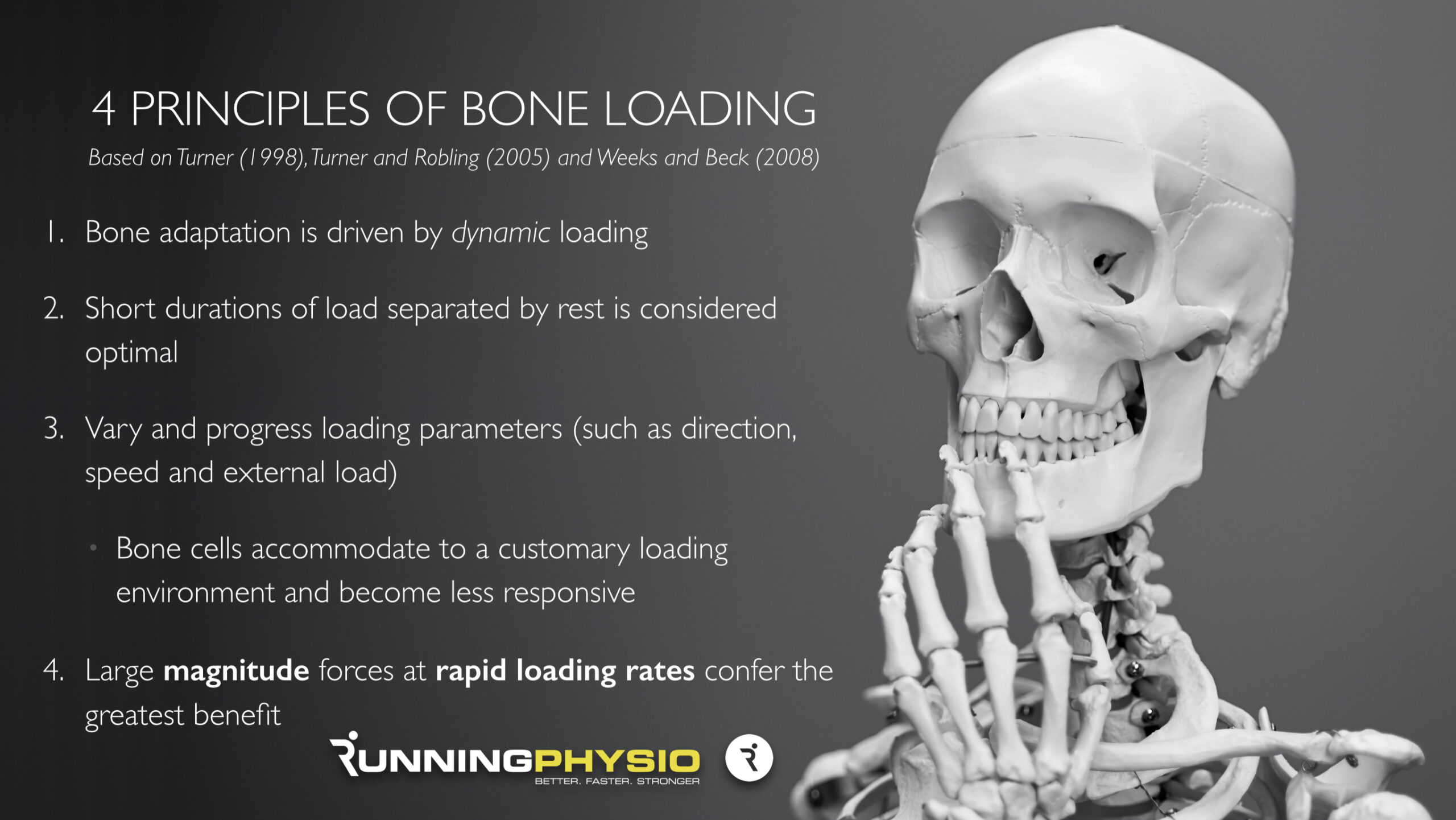
Total number of foot contacts may stay relatively low in rehab of bone stress injury (e.g. approx 40 to 80) as the bone’s ability to adapt to load becomes saturated quickly so more loading cycles doesn’t necessarily result in more adaptation. For more on this, see our 4 principles of bone loading graphic below, from Running Repairs Online.
Additional considerations
We’ve given Ben some indication of reps and sets but also suggested he works to fatigue within each set. The rep range is currently roughly 8 to 12 reps. We’re using fatigue here as a method to ensure he’s loading enough. If Ben isn’t reaching fatigue within this range he needs to make the exercise harder by adding load, increasing range or increasing time under tension. We’ve also suggested Ben works alternate legs – work to fatigue on the right then exercise the left leg while the right leg recovers.
Communication is important here – Ben is happy with his exercises and how to progress each of them. We’ve also discussed them with his S&C coach and kept his running coach up to speed on his progress and load tolerance so we can work together as an integrated team.
As I’ve mentioned in the exercise image above this is not a recipe for MTSS just a snapshot of one patient’s exercises and why we’ve used them. Ben’s rehab is reviewed, adapted and progressed at each session and is part of a comprehensive management programme including athlete education, gait re-training and a graded return to running.
We’ve worked with Ben’s S&C and Running Coaches to develop a programme that allows adequate recovery between strength, plyometric and running sessions.
Closing thoughts: exercise prescription for MTSS and other injuries requires an individualised approach considering how, when and where the athlete might do their rehab. It’s essential too that they know why they’re doing it and how it will help them achieve their goals. Not every patient will want an extensive programme; in fact, in many cases, 3 or 4 key exercises can be very effective. If you prescribe exercises consider doing one of the programmes you’ve provided for a week – it’s much harder than you’d think! My final point is key…
…exercise prescription is all about reasoning not recipes!
This article is intended for informational purposes only and is not a substitute for medical advice. It was written by Tom Goom. For further expert resources and to learn more from him, visit his website at Running Physio.
Want to learn more about bone stress injuries?
Dr Stuart Warden has done a Masterclass lecture series for us on:
“Bone stress injuries”
You can watch it now with our 7-day free trial!

Don’t forget to share this blog!
Leave a comment (1)
If you have a question, suggestion or a link to some related research, share below!
You must be logged in to post or like a comment.
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Thanks for the article! What frequency would you recommend for this exercise program?