
Pseudoscience is rife in the sporting world, with no better example than the myths and fallacies surrounding the not so humble running shoe. Mountains of conflicting research has contributed to the development of “footwear tribes” within the running fraternity, fuelled by personal biases and topped with good lashings of poor critical thinking.
Understanding that human bipedal running is extremely variable and complex suggests that nothing will be clear cut in running injury management.
Research into shoe benefits and running injury (RI) has been enormously heterogenic and heavily retrospective, limiting its usefulness. In fact, designing a running study that is prospective in nature with sufficient power is no mean feat. It is only recently that some prospective studies have been published that can look into causation of running injuries [1,2,3,4]. These studies MAY help us in answering that inevitable patient question:
“What running shoes do you think I should buy?”
To answer that question the clinician must ask themselves:
“What does the research show on injury prevention or management benefits from different types of running shoes?”
In regards to the research base there are two bodies of work:
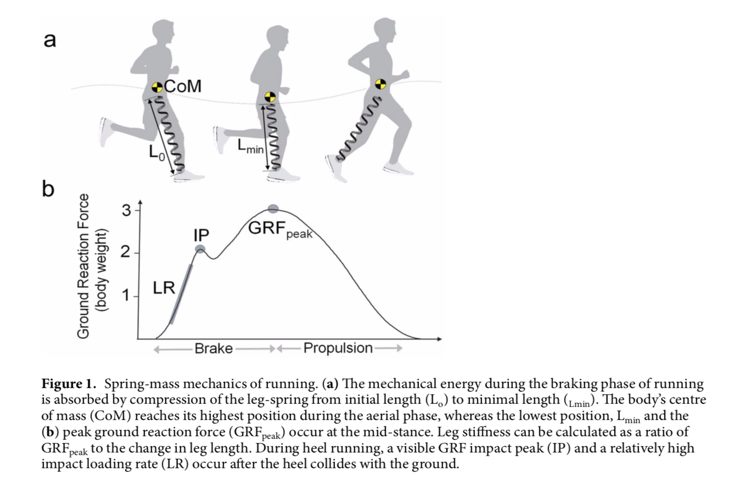
- Biomechanical: Loading Rate (LR), Impact Peak (IP) and Ground Reaction Force (GRF) type studies [5,6]. Impact and pronation became the “villains” in RI, despite the fact biomechanical data can’t be taken as the injury mechanism. The spring-mass mechanics of running are a heavy focus in this body of work [7].
- Sports Medicine: External RI mechanisms from e.g. repetitive overloading due to intensity, volume and frequency training mistakes [4,8,9,10]. Internal mechanisms include psychology and the individual’s physiology.
Spring-Mass System Definition: The cyclical elastic leg behaviour during running which permits efficient force production throughout a stretch-shorten muscle action whist attenuating high energy impacts.
Reference: [7] Kulmala 2018
Biomedical linear thought processes, along with good doses of post hoc ergo propter hoc error, have seen biomechanical data extrapolated directly to causation of injury and shoe design despite no prospective data [11].
Impact Attenuation & Pronation Control Footwear
In the 1980’s, hyper focus on impact attenuation and correcting “excessive” pronation saw a generation of cushioning and control footwear arrive and persist in the running shoe market. Through to the mid 2000’s militaries around the world associated excessively pronated feet with injury risk (some still do), to the point that static foot posture became a screening tool on recruitment. The USA Military has struggled with high RI rates and have performed significant research. It appears that the physically taxing induction training on increasingly unfit recruits is probably introducing several more important injury risk factors that require management [12]. The USA military found “footwear interventions should focus on proper fit and comfort; the evidence does not support running shoe prescription per foot type to reduce injury risk among recruits” [13]. A series of studies on 7000 soldiers found foot type did not influence injury risk, nor did prescription shoeing [14].
In the civilian running population results gained from prescription of expensive orthotics, cushioned and pronation control shoes were also not overly exciting [15,16].
But wait!!! A recent small 2017 prospective cohort study has shown runners with more medial foot pressure in stance experienced more Achilles, medial shin and plantar fascia injuries [2]. Another recent prospective study of 249 female runners found those seeking treatment for their RI had higher vertical peak loads than non- injured runners [1]. These studies support a 2016 SR & meta-analysis finding that tibial stress fractures were associated with a loading rate 12% higher than controls [17]. Further, an interventional study involving subjects and controls wearing identical shoes, except for built in pronation control, found over 6 months that the more pronated subjects with motion control shoes reported lower injury rates [18]. According to this research, the control shoe may be suitable for some pronated patients.
Rearfoot vs Forefoot Strike <– > Shod vs Barefoot
The next evolution were the rear vs forefoot strike studies, which became enmeshed in the shod versus barefoot or more recently minimalist paradigms. Nowhere has pseudoscience with huge doses of confirmation bias been more obvious than in the barefoot running research [19].
In barefoot and minimalist running, proponents argue that variations of forefoot and midfoot strike are encouraged, resulting in [20]:
- Smoothing of the impact peak on the spring mass curve
- Reduced patellofemoral loading
- Less predictable muscle activity patterns
- Improved foot-ground proprioception
- Enhanced elastic recoil mechanisms of the arch & Achilles tendon (note: increased loading)
Classically shod running tends to encourage heel strike which is associated with greater landing impacts than forefoot/midfoot strike. The assumption could then be barefoot or minimalist shoeing should decrease injury rates and improve performance. A 12 week progression into a more minimalist shoe study (neutral->partial minimalist->Vibrams) found increased levels of injury in the partial minimalist shoe and more shin and calf pain in the Vibram group [21]. Training error (too rapid a transition) plus motoric confusion re heel or forefoot strike in the partial shoes could be suspected here.
High Midsole Cushioning – the latest trend
Highly midsole cushioned shoes are a more recent trend, harking back to impact attenuation theory. In late 2018 two biomechanical studies on midsole cushioning were published with seemingly conflicting outcomes.
Kulmala et al [7] investigated “The Shoe Cushioning Paradox” [15,22]. Historical assumption is that cushioning should reduce impact loads. The effect of highly cushioned (Hoka Conquest) vs conventional control (Brooks Ghost 6) shoes at two speeds (14.5 km/h and 10 km/h) was examined. At the higher speed the highly cushioned shoes demonstrated increased GRF impact peak (IP) of 10.7% and increased loading rate of 12.3%. At the slower 10 km/h speed there was a smaller increase in IP of 6.4%.
Midsole cushioning resulted in significant differences in the spring-mass running mechanism, with the runner’s leg stiffening in contact phase. Humans have an adaptive mechanism to maintain the same movement of the body’s CoM across different surfaces by adjusting leg stiffness during the stance phase [15,23,24].
Nigg [25] proposed that bodies have a “preferred movement path” and that changes in shoes and orthotics can change range of motion, but muscle activity keeps the body on the preferred “path”. This is an interesting finding as the running movement appears not to change but the muscle activity/energy demands might be vastly different under different shoe conditions, having implications for shoe prescription. This study also suggested shoe selection should focus on comfort.
Meardon [26] performed a cross-sectional biomechanical study aimed at examining the influence of midsole cushioning over ground in three midsole conditions (3 pairs of NB shoes constructed for each subject with same height but 3 different midsole cushioning densities). Ankle contact force and load rates were decreased with significant effect with more cushioning. Less effect was seen at the knee and hip. They suggested that increasing shoe cushioning 10 to 20% may help individuals to unload the ankle and to a lesser extent the knee and hip (a classic example of inappropriate extrapolation from a biomechanical study!).
So… They’ve Asked You The Question – What Are You Going To Say?
A 2014 systematic review of prospective cohort studies investigating risk factors for RI firmly concluded that the main risk factor was a running injury in the last 12 months[8]. This indicates the need for a thorough physiotherapy assessment and application of clinical reasoning! Patient beliefs are often that shoes will fix the problem, so education is important.
Following are some answers given by a research informed gait lab running physio when discussing shoes with patients:
- “It’s most likely that the shoe prescription is the least important factor”
- “I suspect unloading a bit and checking your training programme is more important than your shoes at the moment”
- “You do tend to take a lot of force on the inside of your feet, so some light built in shoe control there may help”
- “Whilst the metatarsal heals we need to take you out of forefoot strike and minimalist, so go with some more cushioning”
- “You’re heel striking in these barefoot shoes. Do you want to go into a bit more cushioning for a while to ease your heel pain?”
- “You don’t really need all that control, let’s maybe try a little lighter next purchase?”
- “One shoe type doesn’t fit all. Try a few pairs and pick the comfortable ones – don’t look at the sole thickness too much”
- “Just because Eliud Kipchoge runs in Vaporfly doesn’t really mean you need to”
- “There is some evidence to say variability by alternating a couple of different pairs of shoes can help, if you have the finances”
- “Your Achilles is struggling in barefoot, maybe look at a little more heel-toe drop to unload it?”
- “A slightly less steep heel-toe drop shoe for a while may unload your kneecap”
- “A slightly more cushioned shoe may be a good idea whilst your ankle heals”
- “Barefoot and minimalist shoes take quite some time to work into. Your body naturally adapts with loading. You may struggle going straight to barefoot from a conventional shoe. Let’s go in between for the time being”
Want to learn more about running injuries?
Rich Willy has done a Masterclass lecture series for us on:
“Restoring load capacity in the injured runner”
You can try Masterclass for FREE now with our 7-day trial!

References
Don’t forget to share this blog!
Related blogs
View allElevate Your Physio Knowledge Every Month!
Get free blogs, infographics, research reviews, podcasts & more.
By entering your email, you agree to receive emails from Physio Network who will send emails according to their privacy policy.
Leave a comment
If you have a question, suggestion or a link to some related research, share below!